





Disinhibition is one of the main symptoms of the behavioural variant frontotemporal dementia (bvFTD), a type of dementia associated with degeneration of the frontal and temporal lobes of the brain. Patients with bvFTD exhibit behaviours that are considered inappropriate, to the point that caregivers and family members may feel helpless. Thanks to the ECOCAPTURE study conducted at the Paris Brain Institute by Bénédicte Batrancourt, Richard Levy and Lara Migliaccio (Inserm, CNRS, Sorbonne Universities, AP-HP), new avenues are emerging to distinguish different types of disinhibition on which it is possible to intervene without resorting to medication. This could lead to improved care and reduce the isolation of patients and their caregivers. The results of the study are published in the journal Cortex.
The behavioural variant of frontotemporal dementia (bvFTD), like other types of dementia, is marked by a progressive decline in cognitive function. But it is also characterized by severe brain atrophy and the presence of abnormal protein deposits inside neurons. The effects of bvFTD on behaviour are particularly pronounced, and even more troubling as they appear in subjects who are still young and active – between 45 and 65 years old. Changes in personality expression, apathy, impaired judgment and empathy, inappropriate conduct, … The symptoms are difficult to manage since patients are not aware of their disease, and do not perceive its effects on those around them.
“Frontotemporal dementia needs to surface from invisibility. Because patients are not able to seek care, which is common in neurobehavioural diseases, they don’t really have a voice of their own, Migliaccio said. As for caregivers, they often feel at loss because patients are young and rarely have co-morbidities. Nursing homes or hospitals are not appropriate places for them. »
Currently, there is no specific treatment for bvFTD. Sometimes confused with other disorders, such as Alzheimer’s disease, bvFTD is even more difficult to identify when the behaviour of patients is a source of taboo in the family environment. For all these reasons, the disease remains poorly understood – as well as disinhibition, one of its key symptoms. Because the manifestations of disinhibition can be specific to each individual and vary according to the environment and social situations, researchers must study them in a realistic framework, what we call an “ecological” approach.
Expression of disinhibition in context
This is the purpose of the work carried out by Lara Migliaccio and Bénédicte Batrancourt at Paris Brain Institute, within the FrontLab team led by Richard Levy. In collaboration with colleagues at the University of Rennes, researchers recruited 23 bvFTD patients and 24 healthy volunteers at Pitié-Salpêtrière Hospital in Paris. They studied the behaviour of each individual in the same scenario: the participants had to wait, alone, in a furnished room resembling a medical waiting room – equipped with invisible cameras. For 45 minutes, they were invited to explore the room and interact freely with the objects dispatched within it (games, magazines, food, drinks, scales, pens, etc.). In the last part of the experiment, participants were given a questionnaire which required them to explore specific aspects of the room to complete the various questions.
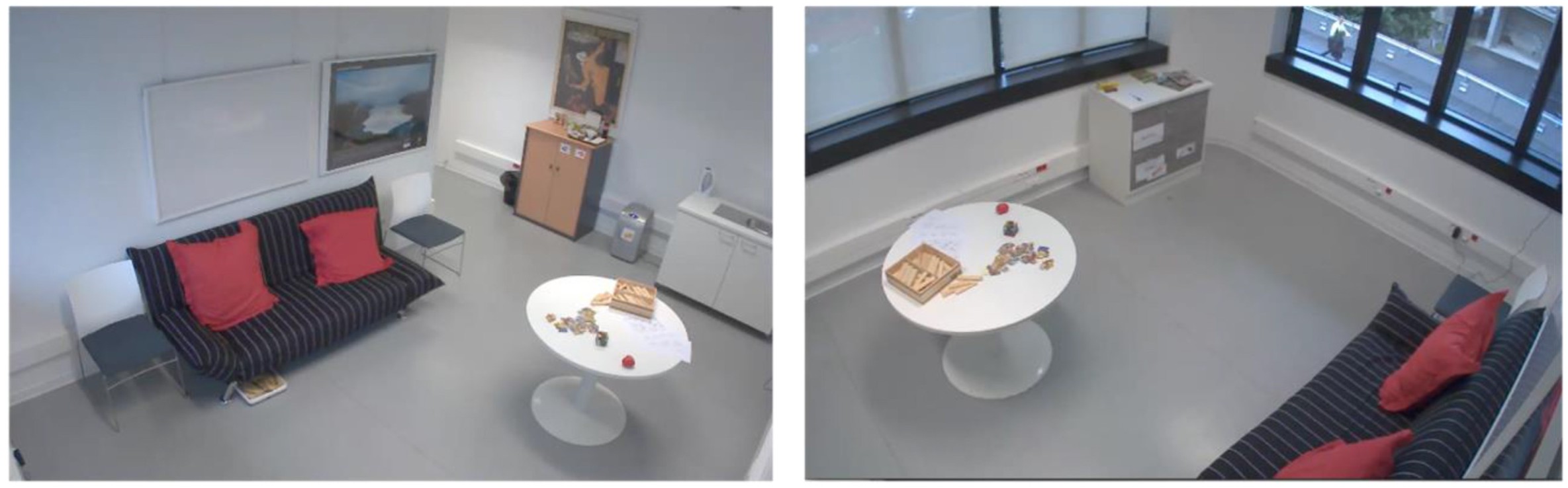
Reconstruction of a waiting room for the ECOCAPTURE study. Credit: FrontLab, Brain Institute.
With this scenario, designed to encourage the emergence of unexpected initiatives, the team observed a variety of disinhibited behaviours in both the bvFTD and control groups. They classified them into three categories: Compulsivity, which includes repeated movements or inappropriate perseveration (opening and closing the window with no particular purpose, rubbing hands continuously, insisting on turning on a tap that doesn’t work… ), impulsivity, marked by the emergence of impulses or strong emotions (shouting, laughing, dancing…) and social disinhibition, in which the participant does not respect implicit social codes of communication with others (non-compliance of the experimenter’s instructions, excessive familiarity, insults…).
This classification allowed the researchers to objectively measure the effects of a third-party intervention on the different components of disinhibition. Their results first indicate that, believing themselves to be alone, all participants showed some level of disinhibition. This was much more pronounced in the bvFTD patients than in the control group, particularly regarding social disinhibition. This finding supports the idea that disinhibited behaviours exist along a spectrum, and that it is simply their intensity and frequency that defines their pathological nature in frontotemporal dementia.
Towards personalised approaches
The researchers also noted that bvFTD patients tended to remain idle if they were not actively encouraged to perform an action. The higher their activity level, the lower their symptoms of social disinhibition. Finally, their level of impulsivity was greatly reduced when they were focused on a task, such as completing the questionnaire requested by the examiner. Stimulation techniques adapted to each patient (games, puzzles, physical activity…) could therefore constitute an efficient non-medicinal approach to reduce frustration and agitation in these patients. Though they are the first to suffer from it, it also affects caregivers and relatives greatly.
These results must now be reproduced on a larger number of patients. Researchers will also have to assess the duration of the benefits induced by the intervention of the caregivers. Indeed, people affected by bvFTD tend to feel more stress when their environment requires cognitive performances that they are not capable of. Inappropriate or intense stimulation could reinforce their symptoms, rather than alleviate them. The authors thus suggest that activities that correspond to pre-existing hobbies, or familiar household tasks (cooking, gardening…) would be most likely to provide significant benefit.
“The next step will be to understand patients’ behaviour in even greater detail, Batrancourt says. The future ECOCAPTURE@HOME program will make it possible to measure variations in their activity level, quality of sleep and emotions according to changes in their environment, at home, thanks to a smart watch. The goal is, in the long run, to personalise care management so that their symptoms can be managed as efficiently and as long as possible at home, as well as reducing any taboo surrounding the disease.“
Thanks to the ECOCAPTURE study conducted with PRISME facility at Paris Brain Institute.
Source
Tanguy, D. et al., Behavioural disinhibition in frontotemporal dementia investigated within an ecological framework, Cortex.
https://doi.org/10.1016/j.cortex.2022.11.013
